*Person Collapses (Adult, assume cardiac arrest)
*Check Responsiveness and Breathing - simultaneously (Tap and Shout) "Are you okay?" - If unresponsive or if pt is not breathing or has agonal breathing, then
*Call emergency response system (call 911 or if in a medical setting call a code blue or retrieve a
defibrillator/AED if available) - the main rhythm associated with cardiac arrest in an adult is V.fib or
Pulseless V. Tach and NEEDS to be shocked as soon as possible to survive.
Begin BLS:
C-CIRCULATION (3 steps):
1. Check responsiveness and for breathing – Tap and shout, "Are you okay?”
Check responsiveness and for breathing – Tap and shout, "Are you okay?”
– look for chest rise – if no response or breathing or
abnormal breathing go to next step
2.Call a Code Blue if in hospital or if out of hospital Call 9-1-1
3.a. Check Circulation- by palpating a carotid/femoral pulse (within 10
seconds). If no definite pulse within 10 seconds then, begin chest
compressions. If a definite pulse is felt, then give 1 breath every 6
seconds for adults and 1 breath every 2-3 seconds for children and
infants. Recheck pulse every 2 minutes or 5 cycles.
b. Provide - CIRCULATION w/chest compressions and ventilations
(30:2) for at least 100-120 compressions per minute, “hard and fast”, at
least 2 inches deep with minimal interruptions. Allow for complete
recoil of the chest after each compression.
A-AIRWAY: Open the AIRWAY using head-tilt-chin lift, if trauma suspected, then use jaw thrust method. Even if trauma suspected and you are the only rescuer available, then open the airway using head-tilt-chin lift.
B- BREATHING: Assessment of this was done in step one - Provide BREATHING (2 breaths) allowing the chest to rise each time, give each breath over 1 second. Avoid excessive ventilations. If the breath does not go in, reposition the head by head-tilt-chin lift and attempt to deliver 2 breaths. Utilizing a bag-valve-mask (BVM) requires a good seal – E-C method, E with 3 fingers along jawbone and C with thumb and forefinger on the mask. Please note that this is best done with 2 rescuerers and not recommended for the single lone rescuer.
Helps arrives and begins D for defibrillation, or if patient has a definite pulse, then skip to the secondary survey.
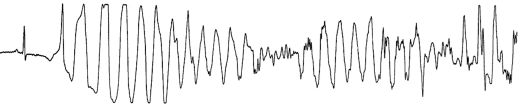
D=Defibrillation, Attach to a defibrillator-monitor or with paddles do a quick look for a shockable rhythm. We are looking for V.fib or V.Tach to defibrilate.
C=Circulaton: Resume CPR with Chest Compressions 30:2
Primary Assessment:
- A=Airway - Is the airway open and patent? If not, secure the an airway with an advanced airway device. Intubate patient with an ET tube or another advanced airway
(see below for different types and for a discussion on intubation)
Continuous waveform capnography is recommended as the
recommended secondary confirming technique and recommended for
maintaining correct placement of the endotracheal tube. Class I.
PETCO2 (partial pressure of end tidal carbon dioxide) normal range is
35-40 mmHg. If < 10 mmHg, in arrest, then improve the quality of
CPR.
- B=Breathing - Are ventilation and oxygenation adequate? Place on oxygen and/or confirm placement with capnography. Once the advanced airway is in place. RR then should be 1 breath every 6 seconds (10 breaths per min) and NOT syncronized with chest compressions. If patient has a pulse and does NOT have an advanced airway, then ratio is 1 breath every 5-6 seconds.
- C=Circulation – Is CPR resumed with chest compressions? Has an (intravenous device) IV been placed? Antecubital vein is 1st choice for peripheral line/IO (intraosseous) route is an acceptable alternative and give medications (Vasopressor) - CPR for 5 cycles/2 minutes - meds (Antiarrhythmic). No interruptions from CPR for more than 10 seconds.
- D=Disability - What is the patient's neurologic funtion? AVPU - Alert, Voice, Pain, Unresponsive
- E=Exposure - Remove all clothing to access for any potential problem.
Secondary Assessment:
SAMPLE=Signs and Symptoms, Allergies, Medications, Past medical history, Last meal eaten, Events (what happened) - look for 5 Hs and 5 Ts: Hypovolemia, Hypoxia, Hydrogen Ion (Acidosis), Hypo/hyperkalemia (low or high K level), Hypothermia, & Tension Pneumothorax, Tamponade-cardiac, Toxins (overdose - see PEA for tx), Thrombosis-pulmonary (Pulmonary Embolism-PE), Thrombosis-cardiac (Myocardial Infarction-MI).
**Note: Pneumonic for those who just want the quick and dirty. Use it if it helps, below is a more in depth discussion of each intervention**
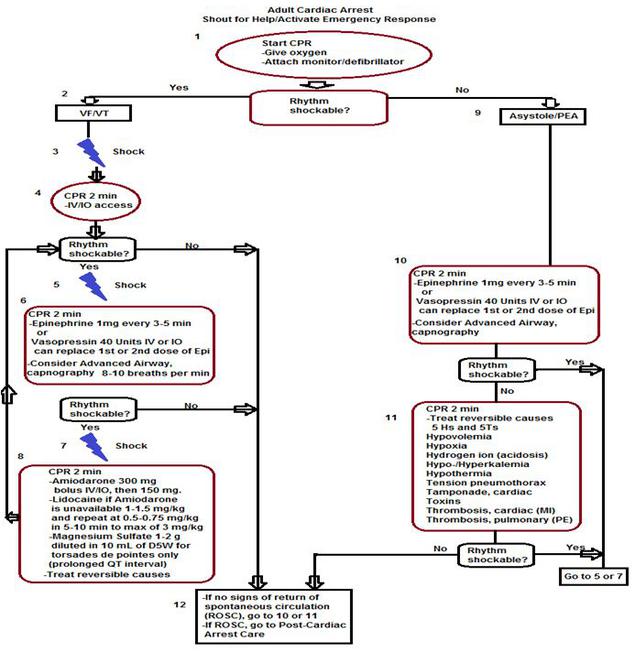
Shock (120 to 200joules - biphasic and 360joules - monophasic)
resume CPR
Everybody Shock, (Epinephrine 1mg IV q3-5min then Shock) - Vasopressin has been removed from ACLS in 2015
And - (Amiodarone 300mg IV push, repeat 150mg in 3-5 minutes)
If amiodarone is unavailable then give
Let's - (Lidocaine 1-1.5mg/kg IV push repeat in 3-5 minutes at half the dose
0.5mg/kg to 0.75mg/kg to a max dose of 3mg/kg)
If pt has torsades de pointes associated with a long QT interval
Move - (Magnesium Sulfate 1-2gm IV over 10 min.)
-----------
(Bicarbonate 1mEq/kg IV push q 10min under certain
circumstances like hyperkalemia, certain drug overdoses, and for some acidotic conditions). It is not recommended to be liberally or prophylactically given.
Precordial Thump. No evidence shows a beneficial conversion from VT to a perfusing rhythm, but some evidence shows a deterioration. Therefore, it is not recommended one way or the other any longer.
D=Defibrillation, Attach to a defibrillator-monitor or with paddles do a quick look for a shockable rhythm. We are looking for Ventricular Fibribllation or PULSELESS Ventricular Tachycardia to defibrillate. Make sure the SYNC button is off.
Place paddles or patches one over apex (~ left side 5th ICS at anterior axillary line) of the heart and the other at right up chest (right sternal border at 2nd ICS.) If using paddles, make sure you use a water soluble gell or two 4x8s moistened with normal saline and use 25 lbs of pressure to prevent arching.
One Shock -Defibrillate one time if needed for persistent Ventricular Fibrillation (V. Fib.) or Ventricular Tachycardia (V. Tach.), in succession, do not stop if rhythm still present with each shock: 120 to 200joules - biphasic or 360joules - monophasic.
*monophasic or biphasic energy may differ, see manufacturer of your AED or Defibrillator for details.
**Remember it is your responsibility to make sure no one touches the patient or anything touching the patient.** Call out: "I'm clear! Your clear! Everyone clear!"
Look at the rhythm after one shock and ask is the patient still in V. Fib. or V. Tach.
If so, then proceed to the Secondary ABCD survey.
C=Circulation, resume CPR with chest compressions first and continue to do CPR for 5 cycles or 2 minutes. Place IV, antecubital vein is 1st choice or Intraosseous access. Administer drugs appropriate for rhythm and condition.
One Shock-Defibrillate 120 to 200joules - biphasic or 360joules - monophasic one time if still in V. fib/Pulseless V. tach.
CPR for 5 cycles/2 minutes. If diastolic pressure during CPR with an arterial line is < 20 mmHg, then CPR quality needs to improve.
Consider a vasopressor:
E in everybody = Epinephrine 1 mg IV q3-5 min.
Flush with 20 mL NS or run IVFs to keep meds running into the vein and raise the arm.
A=Airway-consider placing an advanced airway device. (See Case 1 for a detailed description of each airway device and oxygen recommendations). This provides an airway and a potentially a drug route, although this is very inconsistent as the absorption of medications in the ET tube vary greatly from person to person. Capnography should be utilized with the advanced airway. PETCO2 (partial pressure of end tidal carbon dioxide) normal range is 35-40mmHg. If < 10 mmHg, in arrest, then improve the quality of CPR.
B=Breathing-confirm airway device by exam and capnography waveform monitoring if available, secure the airway with an approved device, and bag pt with 100% oxygen, confirm oxygenation and effective ventilations by chest rise.
After giving the drug, then resume CPR for 5 cycles/2 minutes.
Then, Shock = Defibrillate 120 to 200 joules - biphasic or 360 joules - monophasic
Resume CPR for 5 cycles/2 minutes.
Next, consider antiarrhythmic, Amiodarone.
A in And = Amiodarone 300mg IV push, repeat in 3-5 minutes with 150mg IV. If starting an infusion, run 1 mg/min for 6 hours, then 0.5 mg/min for rest of time with max dose 2.2 grams in 24 hours.
If Amiodarone is NOT available, then try:
L in Let's = Lidocaine
1mg/kg - 1.5mg/kg (quick conversion on weight is take the weight in lbs - then divide by 2.2 = weight in kg. Lidocaine comes in 100 mg syringes). IV push repeat in 3-5 minutes with half the dose (0.5 - 0.75 mg/kg to a maximum of 3mg/kg.
-------
M in Make = Magnesium Sulfate 1-2grams IV over 10 minutes only for torsades de pointes with prolonged QT interval. The rhythm does not get bigger and smaller like seen with polymorphic V. Tach. at times. It twists on its axis. In this picture from http://img.medscape.com/fullsize/migrated/561/317/jce561317.fig1.gif it shows the upright QRS starting out, then the twist and the QRS pointing down, then another twist and it points up again.
-------------------------
I'll explain some of the interventions below with the next step as to how some might fit in earlier in the process.
See PEA algorithm for a detailed description of each.
D=Differential Diagnosis, Search for and treat reversible causes including but not limited to 5 Hs and 5 Ts:
-Hypovolemia-give fluids and/or blood products (the #1 cause of PEA),
-Hypoxia-give 100% ventilated oxygen,
-Hypo/hyperkalemia (low or high K level)-give KCL boluses not more than 20mEq per hour for low K+ level/-give NaHCO3 1mEq/kg IV every 10 minutes for high K+ level,
-Hydrogen Ion (acidosis)- Interpretation of arterial blood gases may be needed here to make a judgement for its use. On the home page, I have a button to PowerPoints one of which is ABG interpretation. Hyperventilating the patient if the patient is in respiratory acidosis (use cautiously) or give NaHCO3 due to certain metabolic conditions and for hyperkalemia and for certain drug overdoses (follow your medical recommendations)
-Hypothermia - Patients with Severe hypothermia (body temperature 30°C [86°F]) associated with marked depression of critical body functions, which may make the victim appear clinically dead during the initial assessment and cardiac arrest can be rewarmed most rapidly with cardiopulmonary bypass. Core rewarming includes warm-water lavage of the thoracic cavity and extracorporeal blood warming with partial bypass. Although warmed IV or IO fluids and warm humidified O2 will help, these measures are not rapid and are considered an adjunct. Unconscious adult patients that were out of the hospital with Ventricular Fibrillation as the initial rhythm be cooled to 32ºC to 34°C for 12 to 24 hours after return of spontaneous circulation (ROSC). Similar therapy may be beneficial for patients with other arrest rhythms.
-Thrombosis Pulmonary (PE)-thrombolytics or surgery to remove the blockage,
-Thrombosis Cardiac (MI)-thrombolytics or surgery to remove the blockage,
-Tension Pneumothorax-needle decompression,
-Tamponade, Cardiac -paracardial centesis,
-Toxins - Used to be called tablets for overdoses. Give NaHCO3 (Sodium Bicarbonate) for certain antidepressants, but be cautious of its use.